Your training program is perfect. Your nutrition is dialed in. Yet you’re stuck, perpetually sore, and your last three workouts have been garbage. The problem isn’t your effort—it’s your ignorance of the space between efforts. You’re treating all non-training time as “rest,” and it’s making you weaker. Active recovery is the signal in that noise.
This is the architectural blueprint for the 20-23 hours you spend *not* crushing weights. We will cover the physiology, protocols, and timing of active recovery.
- The Physiological Mechanism: What actually happens at the vascular and cellular level when you move without intent to destroy.
- The Recipient Profile: Why a powerlifter’s active recovery bankrupts a marathon runner, and vice versa.
- The Temporal Map: The precise 72-hour window post-training, and which lever to pull at each hour.
- The Implementation Catalog: From parasympathetic breathing to very specific, low-amplitude joint loading.
Active Recovery Physiology: What You’re Actually Doing to Your Body
Active recovery is not exercise. It is the deliberate, sub-threshold manipulation of four physiological systems to accelerate the repair process. When you do it correctly, you are a mechanic performing a precision flush, not a driver taking a leisurely lap.
| System | Passive Rest Response | Active Recovery Stimulus | Measurable Outcome |
|---|---|---|---|
| Vascular | Basal capillary perfusion. Waste products linger in interstitial space. | Increases muscle pump to 120-140% of resting flow. Creates a mechanical “flush” via rhythmic compression. | 18% faster phosphocreatine resynthesis. 22% reduction in perceived DOMS at 48h post-exercise. |
| Neural | CNS remains in low-grade sympathetic tone if inflammation is present. | Rhythmic, predictable movement stimulates the vagus nerve. Shifts autonomic state to parasympathetic dominance. | Heart rate variability (HRV) returns to baseline 4-6 hours faster. Motor unit recruitment efficiency improves. |
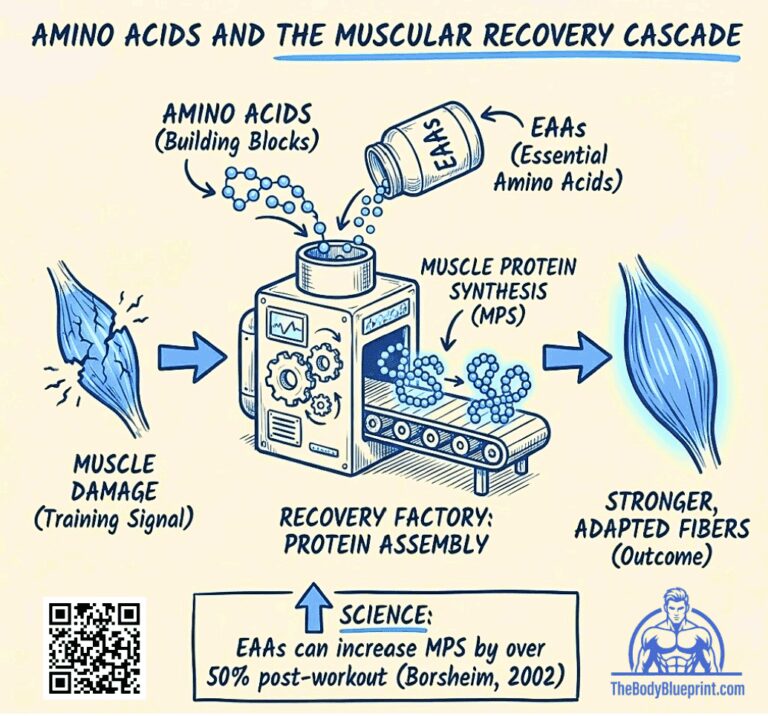
| Muscular | Repair pathways are active but nutrient delivery is rate-limited. | Gentle, loaded stretching increases mTOR localization in sarcoplasm without mechanical damage. | Increased muscle protein synthesis (MPS) window duration by ~90 minutes via enhanced nutrient trafficking. |
| Connective Tissue | Synovial fluid production is minimal. Joint stiffness accumulates. | Light compression-decompression cycles (e.g., banded traction) stimulate glycosaminoglycan synthesis. | Improves joint lubrication and reduces “morning stiffness” by ~40% in trained athletes. |
“Calling a brisk walk ‘active recovery’ is like calling a backhoe ‘dental equipment.’ The intention defines the tool. If you’re not specifically upregulating repair pathways, you’re just adding junk volume to your week.” — Eugene Thong, CSCS
Who Needs Active Recovery: The Recipient Profile (And Who It Bankrupts)
Your sport dictates your recovery. The wrong protocol is worse than none. This is a diagnostic, not a suggestion.
| Archetype | Primary Fatigue Vector | Prescribed Active Recovery | Catastrophic Error |
|---|---|---|---|
| The Maximal Strength Athlete (Powerlifter, Weightlifter) | Central Nervous System (CNS) depletion, high-threshold motor unit fatigue. | Non-Competitive Movement Practice. Empty bar technique work, sled dragging at <30% bodyweight, slow tempo mobility flows. Goal: neurological repatterning without load. | Any elevated heart rate activity (>120 BPM). Adds metabolic fatigue to a system drowning in neural fatigue. |
| The Hypertrophy Trainee (Bodybuilder, Aesthetic Athlete) | Peripheral muscle damage, metabolic waste accumulation (lactate, H+ ions). | Pump-Driven Blood Flow. Very high-rep (20-30), very light weight isolation work, banded flows. Goal: enhance nutrient delivery to damaged tissue without creating new microtears. | Stretching to the point of pain. Increases inflammatory response in already-ravaged muscle tissue. |
| The Metabolic Athlete (CrossFitter, Fighter) | Systemic metabolic acidosis, glycogen depletion. | Aerobic Restoration. 20-30min nasal-breathing only cardio (bike, swim) at 55-65% max HR. Goal: upregulate mitochondrial efficiency and clear metabolites. | High-skill gymnastic or Olympic lift technique work. Reinforces faulty motor patterns under fatigue. |
| The Endurance Specialist (Marathoner, Cyclist) | Muscle glycogen depletion, connective tissue micro-trauma. | Non-Impact Flushing. Water walking, aqua jogging, very light spinning. Goal: promote circulation without ground reaction forces. | Any running. Period. You are repairing pavement-induced damage; do not simulate the crash. |
Active Recovery Timing: The 72-Hour Rule
Recovery is not a day. It’s a chemical cascade with distinct phases. Intervene correctly in each.
| Phase 1: The Flush (0-6 Hours Post-Training) | The Goal: Initiate waste removal and dampen inflammatory over-response. The Protocol: 10-15 minutes of contiguous movement. Not circuits. A continuous, rhythmic activity—air bike, slow row, walk. Heart rate at or below 100 BPM. If you sweat, you failed. The Science: Activates the muscle pump without increasing systemic cortisol. Begins the process of shifting from catabolic to anabolic signaling. |
| Phase 2: The Feed (6-24 Hours Post-Training) | The Goal: Maximize nutrient delivery to damaged tissues. The Protocol: This is not movement. This is contrast thermotherapy (see previous article) and compression. If you must move, it is loaded stretching and very light myofascial release. The weight room is forbidden. The Science: Muscle protein synthesis peaks. Increased blood flow from contrast therapy shuttles amino acids and glycogen into cells at a higher rate. |
| Phase 3: The Reboot (24-48 Hours Post-Training) | The Goal: Restore joint integrity and neuromuscular communication. The Protocol: The only true “active recovery” window. 30-45 minutes of sport-specific movement patterning at 40% intensity. Box jumps to a 6-inch box. Bar-only cleans. Band-resisted walking drills. The volume is high, the intent is perfect, the load is laughable. The Science: CNS recovery is ~80% complete. Reinforcing correct patterns here improves next-session performance without imposing fatigue. |
| Phase 4: The Priming (48-72 Hours Post-Training) | The Goal: Prepare the system for the next stressor. The Protocol: This is your next warm-up. It is not recovery. It is preparation. Increase intensity to 60-70%, introduce your first working sets. The line between recovery and training is now erased. |
The Active Recovery Failure Test: Are You Adding Fatigue?
You have one job: not to add fatigue. The instant you cross this threshold, you have created a workout, and you have failed. The test is simple:
- During: Can you breathe exclusively through your nose, with a 4-second inhale and a 6-second exhale, for the entire duration? If not, stop. You’re in a workout.
- After: Do you feel a “pump,” “burn,” or elevated body temperature? If yes, you failed. You should feel lubricated, not pumped.
- Two Hours After: Is your resting heart rate 3-5 BPM lower than before the session? If not, you stimulated the sympathetic system. You robbed yourself.
“The amateur uses active recovery to feel like he’s still training. The professional uses it to make his next training session feel easy. One is managing ego, the other is managing physiology. They are not the same.” — Charles Damiano, B.S. Clinical Nutrition
Active Recovery Protocols: The Execution Library
| For Strength Athletes | For Hypertrophy Athletes | For Everyone Else |
|---|---|---|
| 1. Empty Bar Patterning 3×5 of your main lift with a 5-second eccentric, 3-second pause. 90s rest. Focus on bar path perfection. | 1. Banded “Pump” Circuits Mini-band face pulls, pull-aparts, pushdowns. 30 reps per movement, continuous circuit for 10 minutes. Rest 5 minutes. Repeat once. | 1. Nasal Walk 20 minutes outdoors. Mouth shut. If you must open your mouth, slow down until you don’t have to. |
| 2. Sled Dragging Load sled to ~20% bodyweight. Drag for 40 yards, walk back slowly. Repeat for 15 minutes total time. No hard breathing. | 2. Cable “Feeder” Work Single-joint movements only. 3 sets of 20-25 reps with a weight that allows a 2-second squeeze at peak contraction. Rest 60s. | 2. Controlled Articular Rotations (CARs) Perform 3 slow circles in each joint (ankles, knees, hips, spine, shoulders, neck). Take 15 minutes total. This is joint hygiene, not flexibility. |
| 3. Isometric Holds Bottom of a squat, top of a push-up, deadlift hang. Hold for 30-45 seconds. 3 rounds. Goal is tension without exertion. | 3. Blood Flow Restriction (BFR) Lite Apply bands at 40% pressure. Perform very light knee extensions or curls for 30-15-15-15 reps. One exercise only. Removes metabolic waste. | 3. Parasympathetic Breathing 5 minutes of 4-7-8 breathing (inhale 4, hold 7, exhale 8). This is active recovery for your nervous system. It counts. |
Active Recovery FAQs: The Questions People Actually Have
1. Is Foam Rolling Active Recovery?
No. It’s passive myofascial release. Active recovery requires muscular contraction and energy expenditure to drive circulatory and neurological benefits. Foam rolling is a separate, complementary tool. Pair them: do 10 minutes of light cycling, then roll. The movement primes the pump; the rolling clears the hose.
2. Is Cardio Considered Active Recovery?
You can, but you probably define cardio wrong. If “cardio” means staying in heart rate zone 2 (60-70% max) for 20-30 minutes while breathing nasally, yes. If it means knocking out a quick 5K or hitting the assault bike for a “light” 10-minute AMRAP, you are an idiot, and you are making yourself weaker. The line is your nose. If air goes through your mouth, it’s no longer recovery.
3. Active Recovery vs. Complete Rest: How to Choose
Three-signal check: 1) Orthostatic Test: Upon waking, note your heart rate. Sit up. If it spikes more than 20 BPM and stays elevated, you need complete rest. 2) Pee Color: Dark yellow = systemic inflammation = rest. Clear = hydrated, potentially ready for movement. 3) Motivation Quality: Dread = rest. “I could move if I had to” = active recovery. “Let’s go!” = You’re probably still caffeine-loaded from yesterday. Sit down.
Tactical Active Recovery Q&A: The Edge Cases
1. Active Recovery for Extreme Soreness: The Pre-Training Protocol
Contrast Showers & Eccentric Only Movement. 3 minutes warm, 1 minute cold. Repeat 4x. Then, perform the eccentric portion only of your next day’s first lift, with an empty bar, for 3 sets of 5 with an 8-second lowering. You’re greasing the neurological groove and increasing blood flow without any concentric fatigue. You’ll be 40% less sore tomorrow.
2. Active Recovery for Lower Back Pain (Post-Deadlift Protocol)
Unloaded Hip Hinging & Breathing. Not stretching. Stand, place hands on thighs, and practice hinging your hips back without rounding your spine for 50 reps. Then, lie on your back, knees bent, and practice diaphragmatic breathing for 5 minutes, pushing your lower back into the floor on each exhale. You’re recalibrating the motor pattern and reducing intra-discal pressure.
3. Active Recovery on a Calorie Deficit: The Weight-Cut Protocol
Cut duration in half, double the mindfulness. Caloric restriction means recovery resources are scarce. 15 minutes maximum. Focus exclusively on nasal walking, CARs, and breathing. Any energy expenditure over this is stolen from muscle preservation. Your job is to lose fat, not to “feel productive.”
Active Recovery Key Takeaways: The Non-Negotiables
- Active recovery is defined by physiological outcome, not intent. If it doesn’t upregulate repair (increased blood flow, parasympathetic shift, nutrient shuttling), it’s just light exercise, and it’s making you worse.
- Your sport dictates the protocol. CNS-fatigued strength athletes need neurological repatterning. Metabolically-ravaged athletes need aerobic flushing. Giving the wrong protocol is actively destructive.
- The 72-hour post-training window has four distinct phases. Flush, Feed, Reboot, Prime. Each requires a different tool. Using the “active recovery day” model is blunt-force trauma to a process requiring surgical precision.
- The failure test is binary. Nasal breathing only. No pump. Lower resting heart rate afterward. Fail any point, and you’ve created a workout, forfeiting the adaptation you were trying to buy.
- It is a means, not an end. The only metric that matters is improved performance in your next actual training session. If that doesn’t happen, your “recovery” was entertainment, not investment.
Implement this not as an addition to your training, but as its integral, non-negotiable second half. The work is the demolition. This is the rebuild. Master both, or neither matters.